In this lesson, you will learn pathophysiology and etiology of pneumonia, the subjective and objective data of a nursing care plan, and nursing interventions and rationales. You will also learn how to write a nursing care plan for pneumonia. This includes making an assessment, the concepts of making a diagnosis, formulating a care plan, writing an implementation list, and making a proper evaluation.
After completing this lesson, nursing students will be able to:
Discover why over 360,000 future nurses turn to NURSING.com as the trusted hub for nursing school success.
Clear and concise study tools to get you from pre-nursing school to NCLEX® success.
Video Lessons, Cheatsheets, Practice Questions, Examples, and More.
For less than you spend on vanilla lattes!
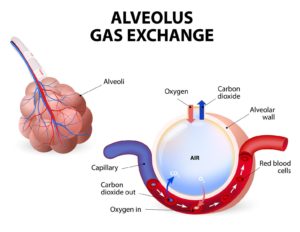
is an infection that causes inflammation of the small air sacs of the lungs, called alveoli, and the surrounding tissue. The inflamed alveoli will fill with purulent material (fluid or pus) impairing their ability to exchange gases with the surrounding capillaries.
Any infectious organism, bacteria, or fungus that reaches the alveoli is likely to be very hostile and will cause them to inflame and fill with fluid. As these fluids build, the lungs ability to exchange oxygen and carbon dioxide is restricted.
In response to the inflammation and fluid build-up the patient will experience:
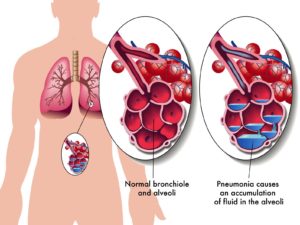
The first picture below depicts a normal, unobstructed gas exchange. In the second picture, the alveoli have an accumulation of fluid in them which impairs the gas exchange that occurs with the capillaries and provides appropriate oxygenation into circulation.
As a nurse, knowing the type of pneumonia is essential for creating a care plan. Pneumonia can be classified in three different ways:
There are four generally recognized kinds of pneumonia based on the setting where they occur:
Community-acquired Pneumonia (CAP) Pneumonia is acquired in the community, not in a healthcare facility. Hospital-acquired Pneumonia (HAP) Pneumonia is diagnosed 48 hours or more after hospital admission. Healthcare-acquired Pneumonia (HCAP) Pneumonia that presents within 90 days of hospitalization, nursing home, or long-term care facility stay, or after receiving chemo or wound care. Ventilator-associated Pneumonia (VAP) Pneumonia is acquired 48 hours or more after endotracheal mechanical ventilation. Aspiration Pneumonia Occurs when food, drink, vomit or saliva is inhaled into the lungs.
There are three general types of pneumonia based on the location in the lung where they occur:
Lobar pneumonia Affects one or more entire lobes of a lung. Also known as non-segmental pneumonia or focal non-segmental pneumonia. Bronchopneumonia Affects distal airways and alveoli in a patchy pattern. Interstitial pneumonia A rare disorder that affects the tissue that surrounds and separates the alveoli.
Symptoms of pneumonia begin when the inflammation and fluid-filled alveoli cause coughing (often producing phlegm), fever, chills, chest pain or pain when coughing, and cold or flu-like symptoms. These symptoms can vary from mild to severe. Mild signs are often similar to a long-lasting cold or flu. More severe cases can include high fevers, organ failure, and even death.
Pneumonia can affect anyone, however those with the following conditions are at greater risk:
Complications of untreated or under-treated pneumonia include respiratory failure, sepsis, metastatic infections, empyema, lung abscess, and multi-organ dysfunction.
Pneumonia can be caused by a virus, bacteria, fungus, or from inhaling something (chemical, inhalant, or aspirating on food or fluid).
Resolve the infection, optimize gas exchange, minimize impact from the impaired gas exchange.
A Nursing Care Plan (NCP) for pneumonia is one of the most common assignments in nursing college. They start immediately after a patient is admitted and document all activities and changes in the patient’s condition. These plans are intended to help enhance quality outcomes and consistent health care delivery. They can also be used as a communication tool among nurses, other healthcare professionals, the patient and their families.
The goal of an NCP is to create a treatment plan that is individualized for the specific patient. They should be anchored in evidence-based practices and accurately record existing data and identify potential needs or risks.
Making an individualized assessment begins by focusing on the available background information of the patient: health history, current health status, psychological state, and other available data.
Subjective data is information or symptoms reported by the patient. These include feelings, perceptions, and concerns obtained by interview. In the case of pneumonia, a patient might report feeling:
Objective data is observable and measurable data, or signs, obtained through observation, physical examination, and laboratory or diagnostic testing. In the case of pneumonia, a patient may present with:
A nursing diagnosis is the basis for establishing and carrying out a nursing care plan. After performing a proper assessment, formulate a nursing diagnosis based on problems associated with pneumonia. This will be your clinical judgment about the patient’s health conditions or needs.
Select the appropriate nursing diagnostic label from the NANDA-I list of approved nursing diagnostic statements that best identify with pneumonia. One or more nursing diagnoses may be given.
Care plan goals form the basis of a nursing intervention. These goals are best thought of as “what the patient will do” and should be a clearly stated, easy to measure, realistic description of the patient’s expected outcomes.
In the case of pneumonia, a plan may include:
Implementations are actions and activities you will take to achieve the nursing plan goals.
These interventions should take into account:
In the case of pneumonia an implementation may include:
The evaluation of our nursing plan involves an organized, ongoing, and intentional assessment of the achievement of set goals and desired outcomes. The evaluation helps determine whether to continue, stop, or change the selected interventions.
In our pneumonia example, our evaluation might include:
| Nursing Intervention (ADPIE) | Rationale |
|---|---|
| Obtain appropriate labs (antibiotic troughs, sputum cultures, ABGs, etc.) | Gives us a baseline; identifies pathogens, and enables us to evaluate if interventions are effective |
| Complete a full respiratory assessment to detect changes or further decompensation as early as possible, and notify MD as indicated | Enables quicker interventions and may change them (for example, wheezing noted on auscultation would potentially indicate steroids and a breathing treatment, while crackles could require suctioning, repositioning, and potential fluid restriction) |
| Promote normothermia (warm patient if the hypothermic, cool patient and administer antipyretics if hyperthermic) | Normothermia optimizes oxygen consumption |
| Cluster care | Activity intolerance is common because of decreased gas exchange; cluster your care to conserve your patient’s energy for essential tasks like ambulation, coughing, and deep breathing, and eating |
| Promote airway clearance | We want to encourage coughing to remove phlegm; do not suppress cough unless clinically indicated. If the patient is able to clear their own airway, continue to encourage this. If not, suction frequently and consider an advanced airway to ensure a patent airway, which ultimately maximizes gas exchange. Getting phlegm out is important. |
| Optimize fluid balance | Patients with pneumonia may not be consuming adequate oral intake due to fatigue or not feeling well, but hydration is essential to healing. Patients may need IV fluids if PO intake is inadequate. |
| Assess and treat pain | If patients are not coughing because of pain, it will only allow fluid to continue to build. Treat pain appropriately and encourage them to cough to clear phlegm. |
| Encouraging coughing and deep breathing | Coughing and deep breathing encourages expectoration, which enables better gas exchange |
| Promote nutrition | Patients with pneumonia typically tire easily and have poor appetites, but need appropriate nutrition and hydration to heal |
| Administer supplemental oxygen as appropriate | Due to the impaired gas exchange, oxygen doesn’t make it into circulation as easily. Providing additional oxygen supports this as much as possible. Use caution in patients with underlying lung conditions. |
| Ensure patent airway | If a patient has unmanageable secretions or is unable to maintain consciousness and keep their airway clear, they must be supported (positioning, advanced airway, etc.) to ensure adequate oxygen delivery |
| Promote rest | Energy conservation is essential; patients should focus on breathing, providing self-care, coughing/deep breathing, and ambulation. Patients cannot adequately participate in these important activities if they are not maximizing their time to rest. Appropriate sleep promotes healing. |
| Administer antibiotics in a timely fashion, draw troughs appropriately | Patients may be on antibiotics, therefore it’s essential to ensure they are administered at the appropriate time and not delayed, as this will impair their efficacy. Also, trough levels will most likely be ordered to assess if the patient is getting too much, too little, or just enough of the antibiotic. The timing of these labs related to administration times is essential for accuracy. |
| Prevent further infection | Patients may have invasive lines like an internal urinary catheter, central venous catheter, endotracheal tube, and so forth. It is essential to care for these devices properly to prevent further infection. |
| Educate patient and loved ones on the importance of energy conservation, effective airway clearance, nutrition, as well as coughing and deep breathing | Patients must be aware of how these aspects of recovery are pertinent so they will be more likely to participate and remain compliant. |
When you start a FREE trial you gain access to the full outline as well as:
“Would suggest to all nursing students . . . Guaranteed to ease the stress!”
Let's work through an example Nursing Care Plan for a patient with pneumonia. The first step is to gather all information. In these examples, we're using a hypothetical patient and we're just assuming that the only problem they have is pneumonia.
In theory, even with this, you'd have all of this extra information, but right now we're just going to talk about relevant information for a pneumonia patient. So what kind of subjective data would we have?
Here's a patient who has pneumonia. What are they telling you?
Well, they might tell you that they are short of breath and maybe they have had a fever. So their temp is high. That's objective and chills, right? Chills are subjective.
Maybe you're noticing that they're having this increased work of breathing and working really, really hard, or their respiratory rate is really high. Maybe they have a cough that you can actually hear, or possibly they reported one. Either way you're going to see sputum, and especially if they've got a bad pneumonia and it's infected, you're gonna see green sputum, which is gross.
You might hear some ronchi because, remember what's happening in pneumonia: they have a ton of fluid in their lungs, might even have an infection. So you're going to hear some ronchi. You might even hear some wheezing.
Of course this patient's gonna be exhausted. If you've ever had pneumonia, you know that you're really, really tired. If they're having really low oxygen levels, then you might actually also see some decreased LOC.
When you're gathering information on a patient, you're also gonna have bowel sounds and urine output and you're also gonna have a blood pressure and all of this other information. Part of putting together a care plan is picking out the relevant information, which is part of step two.
Step two is to analyze the information. And so we're just going to go ahead and say we've analyzed, we've determined we don't need this. This is the information we're looking at specifically for a patient with pneumonia. So we analyze the information, we gather everything and we decide what of the things I've come up with - actually a problem?
We have a patient with pneumonia. So what's their problem? Well, their problem is they have an infection in their lungs, right?
They've got all this fluid and possibly even infection. That of course puts them at risk for something like Sepsis, right? If the infection gets too bad, they can definitely get a lot worse.
Let's see, what other problems do we have while we have that ronchi and all that extra sputum. We've got all those extra secretions in the airway, right? So these are problems.
This is a significant problem for this patient. And we saw that their SpO2 was low. So what needs to be improved is their SpO2, their SpO2 level is really low and I'd like to see it higher, right?
Really we're just analyzing what's actually a problem, what's going on with this patient, what do we need to fix and what can we do.
Then we're going to establish priority. Well, listen, as easy as it is, guys, we can just go ABCs here, right?
This is an infection. This is the airway, this is oxygenation, which has to do with breathing a little bit.
Airway comes first right? So that just makes our life a whole lot easier because the ABC's always happen. Keeping their airway protected, allowing them to get the oxygen that they need, that's definitely going to be our priority.
Now we can ask our “how questions”. So for each one we're going to ask how we knew it was a problem. And this is just where we start linking our data together. So we're going to link our data, we're going to link specific data to a specific problem and then give it a specific intervention.
That's where we talk about how we're actually going to address the problem. So I have a patient, they have a ton of secretions, they have ronchi in their lungs, they have an infection in their lungs and their oxygenation is poor. So what kinds of things am I going to do?
Well, I can give them oxygen, right? I'm probably going to monitor their oxygen as well. Monitor SpO2.
I can do some sputum cultures and then give antibiotics after that, right? To try to treat that infection. Um, maybe I can encourage them to cough and deep breathe cause that's going to help them clear those secretions out. Right?
What other things can we do for those two to help open their airways? Can we do incentive spirometers right? That's going to help open up their airway. I can monitor their airway clearance. Remember, they're fatigued. So what if I would actually promote rest, because they're gonna be really tired. They're not gonna be oxygenating well. So clustering my care, promoting rest, that's going to be really helpful.
These are all little things that we can do for this patient to try to address those problems we already identified. And then how are we going to know it gets better?
Well, one of the big things we said was the problem was their airway clearance, right? So maybe we say they have a patent airway or they're able to clear their own airway. Right?
What about that oxygen level? We can say that their SpO2 increases or maybe that it's greater than 92, whatever your goal is that you want to set for your patient. And then we talked about their infection, didn't we?
They were a little bit worried about the fact that they have an infection. Um, and so maybe we could say that their signs and symptoms of infection decrease or maybe just that they don't develop sepsis. That's always a good thing, right?
These are all things you know, ronchi. So I could say their lungs are clear. There's a lot of things I could do that would give me evidence that this patient is better or that my interventions are working.
From there we're going to translate, we're going to get it into the terms that we need to use and we're going to be able to concisely communicate what the problem is for this patient. And again, here at NURSING.com, we love to use nursing concepts because we think they give you big picture priorities instead of forcing you to drill down to really, really specific issues.
Just use whatever you are required to use if there's something specific. Otherwise just come up with some top things. For this case we said the Airway was our biggest issue, didn't we? So we said I think our number one would be airway clearance, right? If a ton of sputum, a ton of secretions, they've got ronchi in their lungs, we really need to make sure their airways are open because if you give oxygen to somebody with a closed airway, it doesn't do anything for them, does it?
Speaking of oxygen, I would say that oxygenation is probably our second issue. If I have a ton of fluid in my lungs, um, I'm not really going to be able to oxygenate appropriately. So I would say that we could fairly say that's our second problem. And we know with pneumonia, oftentimes there's infection involved. So I think it's fair to say infection control would be another problem.
Here we are, we've translated it, we've said, all right, my top three priorities for this patient are airway clearance, oxygenation and infection control. So now we take those top things and the information we've gathered. And We link everything together. We're able to link our specific problem to the data, to the intervention, to the rationale, and to the expected outcome for that intervention.
Again, we said our primary problems are airway clearance, oxygenation and infection control. Let's take everything we just talked about and let's just transcribe it. We're just getting it on paper.
We're concisely communicating it in one place.
So what tells me that I have a problem with airway clearance. My patient has a cough, they have a lot of secretions. Um, and I have heard ronchi in their lungs. And again, you might've heard ronchi, you might've heard wheezes either way. If you've got airways filled with fluid and secretions, then we can't get the oxygen in it. All right?
So first thing is clear out the airway, then we give the oxygen. So what am I going to do?
We kind of talked about this already. I'm going to assess that cough. I'm going to make sure that it's getting better. I'm going to make sure it's improving. I'm going to assess those lung sounds and I'm probably gonna use an incentive spirometer. And I might even use, um, turn cough, deep breathe. I might even just encourage that cough, because it really helps them to clear those things out of their airway. I know coughing can be very uncomfortable, especially in these moments where you've been coughing and coughing and coughing. But telling your patient, Hey, if we can cough and get this stuff out, you're gonna feel a lot better.
Increased sputum means increased risk for aspiration, but also just poor oxygenation, right? So we need to be able to assess whether or not they have improved or worsened. And we can't do that if we don't assess, right?
That's why we're gonna make sure we do those assessments. And then we do things like an incentive spirometer or turn cough, deep breathe to help open up the lungs and open up the airways. Encourage coughing and clearing secretions. So expected outcome.
Again, we're still talking about airway clearance here, right? This is where we link everything. We line everything up. So expected outcomes.
My patient has a patent Airway, my patient can clear their own secretions and my lungs are clear to Auscultation, CTA, clear to auscultation. So again, we're just lining up our data and our priorities here. We've already gathered everything. Now we're just putting it on paper.
Oxygenation data, my SpO2 was low. Maybe they had a high respiratory rate or work of breathing because their body's like, oh my gosh, give me more oxygen. Right?
And that fatigue, a lot of times that fatigue is caused by Hypoxia. So what are we going to do? Well, we're going to assess that respiratory rate. We're going to watch that SpO2, we're going to promote rest.
We're going to cluster our care because of this fatigue, because again, it's just exhausting to not have enough oxygen.
Um, and then we're going to give oxygen if we need to. This PRN is as needed.
Make sure that you know what your orders are, um, so that you know what you're aiming for, right?
Get provider orders for oxygen if you don't have them. So why do we do the assessments?
Well, we need to track progress and how they're doing. We see fatigue with low oxygen like we said, so that's why we're going to promote rest and cluster care. And then of course giving supplemental oxygen is going to help keep that SpO2 up. So what are our expected outcomes?
Again, we're just linking data, right?
So I want to see that respiratory rate within normal limits. I want my patient to tell me they feel better, right? Report decreased work of breathing, report decreased fatigue and I want to see that SpO2 stay above 92 so all of these are things that are going to tell me that this is no longer a problem.
All of these things are going to tell me that this airway clearance is no longer a problem. All right, last one. Infection control. Patient had fever, chills, we saw green sputum and hey, we may even have seen an increased white blood cell count or an x-ray that was whited out with fluid in the lungs, right?
There's a lot of things that could have told us there was infection happening. So what am I going to do?
I'm going to check cultures. I always do cultures first, right? Because if I give antibiotics before I do cultures, I'm going to skew the results, right?
So cultures I'm going to give antibiotics, I might give antipyretics for that fever and I'm going to monitor their symptoms. I want to make sure that they're getting better. So again, rationales - cultures to determine the organism, antibiotics and antipyretics to treat the infection and the symptoms and monitor temp because we really want to make sure that we are controlling that fever.
So decreased signs of infection, no signs of Sepsis, cause that would be bad. That would mean they progressed and got worse. And we want to make sure we get their temp to within normal limits. Now, normal is relative, make sure you know what your targets are either for your facility or from your provider.
So just to recap on the five steps of writing an excellent nursing care plan, collect all your information, analyze that information, pick out what's relevant to that patient or those problems that you have determined.
Plan your interventions and figure out how you're going to evaluate them. So that's asking your how questions and then translate it, put it into whatever terms you need to use, transcribe it, get it on paper, use whatever form or template you prefer or you need to use. Just get it on paper. Again, remember we are just looking at this isolated pneumonia patient where pneumonia is the only problem that they have.
Remember that it might be that they have pneumonia, but they also have hypertension and they also have a pressure ulcer. And so you can look at every piece of information you have, all of your assessment data, and then determine your priorities. Airway and oxygenation is still probably gonna be at the top, but it's probably more important that I, you know, assess or you know, prevent them from getting a worsened pressure ulcer than it is that I educate them on coughing and deep breathing. Right?
So there's definitely going to be crossover priorities for this, but for this case, this was just a patient with isolated pneumonia.
I hope that was helpful.
Definitely check out the rest of the examples of nursing care plans and check out our nursing care plan library, 130 plus nursing care plan examples.
All right, guys, go out and be your best selves today and as always,
Happy Nursing!
When you start a FREE trial you gain access to the full outline as well as: